


Imagine waking up to an unexpected “calling card” on your back door – an ear print. Such an incident might prompt immediate thoughts about home security, but it also highlights a fascinating truth: the human ear, often taken for granted, is a marvel of biological engineering and a surprisingly unique identifier. Far more than just the visible appendage, this complex organ plays a pivotal role in two of our most vital senses: hearing and balance, profoundly shaping our interaction with the world.
Like any essential piece of equipment in your home, understanding the intricate workings of your ears is crucial for appreciating their function and recognizing potential issues. From capturing the softest whisper to maintaining your steady gait, the ear operates as a finely tuned system. It’s an organ whose design, development, and capabilities are astonishingly sophisticated, allowing us to navigate, communicate, and perceive our environment in ways we often don’t consciously acknowledge.
In this comprehensive guide, we will embark on an in-depth journey through the human ear, dissecting its three main parts, exploring how it processes sound and maintains balance, and tracing its remarkable development from embryonic stages. We’ll also shed light on common conditions like hearing loss, empowering you with the knowledge to better understand and care for this invaluable sensory organ.
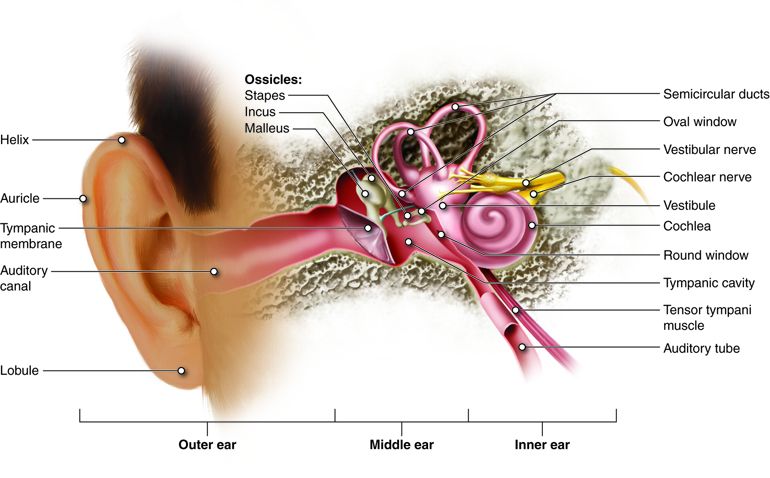
1. **The Outer Ear: Your Visible Guardian**The outer ear, the most recognizable part, serves as our initial interface with the soundscape around us. This external portion includes the fleshy visible auricle, the ear canal, and the outer layer of the eardrum, also known as the tympanic membrane. While often colloquially referred to as “the ear,” this visible structure, the auricle, is merely the entryway to a much more complex system nestled within.
The auricle itself is a cartilaginous structure with a complex relief. It features a curving outer rim called the helix and an inner curved rim known as the antihelix. Further enhancing its intricate design are the tragus, which partially obscures the ear canal, and the facing antitragus. The hollow region in front of the ear canal is termed the concha, all meticulously shaped to guide sound effectively.
Extending inwards from the auricle, the ear canal plays a crucial role in directing sound waves towards the eardrum. This canal stretches for approximately 1 inch (2.5 cm), with its initial segment supported by cartilage and the deeper part, closer to the eardrum, surrounded by bone. This bony section is specifically known as the auditory bulla and is formed by the tympanic part of the temporal bone, providing a robust pathway for sound.
Within the ear canal’s skin are specialized ceruminous and sebaceous glands responsible for producing protective earwax. This natural substance is vital for the ear’s health, as it functions as part of a self-cleaning system, naturally migrating outward through the ear canal. This continuous process helps to clear debris and protect the delicate inner structures from external elements.
While two sets of muscles, intrinsic and extrinsic, are associated with the outer ear, their effect in humans is minimal, unlike in some mammals that can adjust the direction of their pinna. Sensation to the outer ear and surrounding skin is intricately supplied by a network of nerves, including the facial nerve, the great auricular nerve, the auricular nerve, the auriculotemporal nerve, and the lesser and greater occipital nerves of the cervical plexus. This detailed innervation highlights the ear’s sensitivity and its integration with broader neurological pathways.
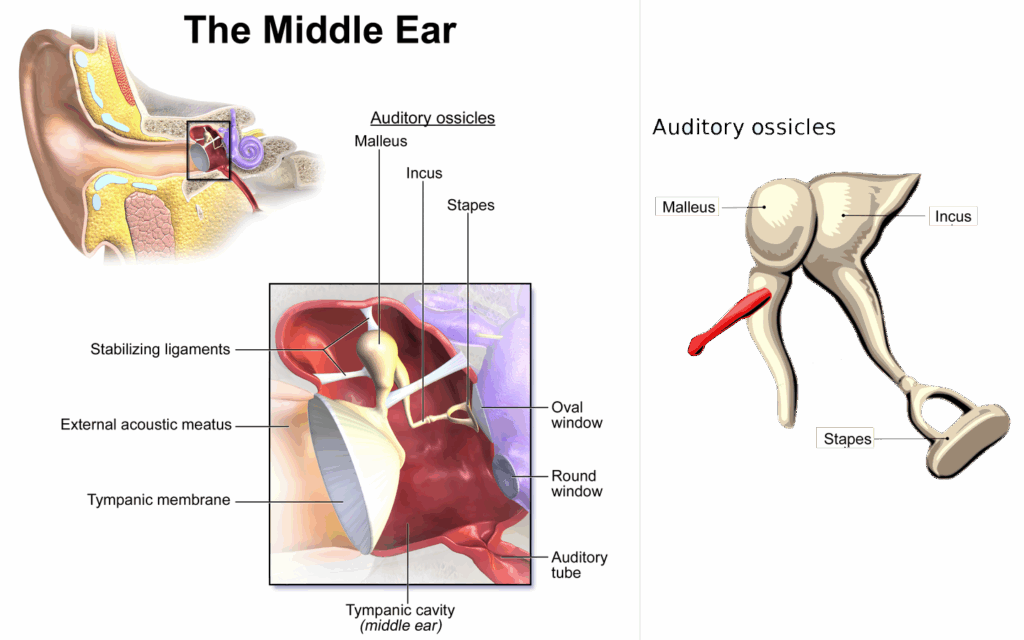
2. **The Middle Ear: Amplifier and Transmitter**Positioned strategically between the outer and inner ear, the middle ear is an air-filled cavity known as the tympanic cavity. This crucial chamber houses the three smallest bones in the body, collectively called the ossicles, along with their attaching ligaments, the auditory tube, and the round and oval windows. The meticulous arrangement of these components is essential for the transmission and amplification of sound from the external environment to the inner ear’s sensory structures.
The three ossicles — the malleus (hammer), incus (anvil), and stapes (stirrup) — are marvels of microscopic engineering. They are designed to work in concert, receiving vibrations from the eardrum, amplifying them, and then transmitting this enhanced sound to the inner ear. It is noteworthy that the stapes, in particular, holds the distinction of being the smallest named bone in the human body, underscoring the delicate precision of this system.
The process of sound transmission begins when sound pressure causes the eardrum to vibrate. The malleus, connected at its longest part (the manubrium or handle) by a ligament, receives these vibrations. It then faithfully transmits these mechanical movements to the incus, which, in turn, passes them along to the diminutive stapes bone. This intricate chain reaction ensures that the sound energy is efficiently transferred and prepared for further processing.
Crucially, the wide base of the stapes rests precisely on the oval window, the gateway to the inner ear. As the stapes vibrates, these movements are transmitted through the oval window, initiating a wave of fluid movement within the cochlea, a key structure of the inner ear. This mechanical leverage provided by the ossicles is highly effective, allowing them to amplify sound waves by a factor of nearly 15 to 20 times, making fainter sounds audible and clearer.

3. **The Inner Ear: Command Center for Sound and Balance**The inner ear, deeply embedded within the temporal bone, represents the ultimate command center for both hearing and body balance. This complex cavity, known as the bony labyrinth, contains structures critical for multiple senses. A central area, termed the vestibule, houses two small fluid-filled recesses: the utricle and saccule, which are fundamental for maintaining static balance. These vestibule structures connect seamlessly to the semicircular canals and the cochlea, forming an integrated sensory unit.
The inner ear is distinguished by its intricate components, each with a specialized role. There are three semicircular canals, uniquely angled at right angles to each other, which are primarily responsible for dynamic balance – sensing motion and acceleration. Alongside these, the cochlea, a marvelously spiral shell-shaped organ, is exclusively dedicated to the sense of hearing. Together, these sophisticated structures, filled with specialized fluids, constitute the membranous labyrinth.
Structurally, the inner ear’s journey begins at the oval window, which receives the amplified vibrations from the incus of the middle ear. These vibrations are then transmitted into the inner ear, specifically into a fluid known as endolymph, which fills the membranous labyrinth. The endolymph is distributed within the utricle and saccule, and subsequently, it flows into the cochlea, initiating the process of converting mechanical energy into neural signals.

4. **The Marvel of Hearing: How Sound Reaches Your Brain**The journey of sound from an external source to our conscious perception is an astonishing display of biological engineering within the ear. Sound waves first travel through the outer ear, where the pinna helps to focus and direct them. These focused waves then impact the eardrum, causing it to vibrate. This initial mechanical energy is the first step in a complex sequence that ultimately registers as sound in our brain.
From the eardrum, the three ossicles of the middle ear – the malleus, incus, and stapes – come into play. The malleus rests on the eardrum membrane and receives its vibrations. This vibration is then efficiently transmitted along the incus and stapes to a second, much smaller window, the oval window. This ossicular chain is not just a passive conduit; it actively amplifies the sound waves, preparing them for the fluid-filled environment of the inner ear.
Furthermore, two small muscles, the tensor tympani and stapedius, are integral to modulating noise within the middle ear. These muscles reflexively contract to dampen excessive vibrations, protecting the delicate inner ear structures from potentially damaging loud sounds. This protective mechanism is a testament to the ear’s sophisticated self-regulation, ensuring the longevity and health of our auditory system.
The vibration of the oval window sets in motion the endolymph fluid within the vestibule and the cochlea of the inner ear. As these fluid waves move, they flow against a specialized sensory epithelium studded with hair cells located in the organ of Corti. These microscopic hair-like structural protein filaments project into the fluid, and their movement is the critical moment of transduction.
When the fluid pushes against the filaments of individual hair cells, it causes ion channels within the receptor cells to open, allowing potassium-rich endolymph to enter. This influx of ions leads to the depolarization of the cell, generating an action potential. This electrical signal is then transmitted along the spiral ganglion, which subsequently sends this vital information through the auditory portion of the vestibulocochlear nerve to the temporal lobe of the brain, where it is finally interpreted as the sounds we hear. The human ear, with its remarkable sensitivity, can generally perceive sounds with frequencies between 20 Hz and 20 kHz, a testament to its broad auditory range.

5. **Maintaining Your Equilibrium: The Ear’s Role in Balance**Beyond its renowned function in hearing, the ear performs an equally critical role in maintaining our body balance, both when we are moving and when we are stationary. This intricate capability is facilitated by the vestibular system, a complex network within the inner ear that provides two distinct types of balance: static balance and dynamic balance. These mechanisms work in concert to ensure our stability and spatial orientation.
Static balance, which allows us to perceive the effects of gravity and maintain our posture when at rest, is primarily provided by two small ventricles within the inner ear: the utricle and the saccule. The cells lining the walls of these ventricles are equipped with fine filaments, and these cells are covered by a delicate gelatinous layer. Each of these sensory cells boasts between 50 and 70 small filaments, along with a single, larger filament known as the kinocilium, all poised to detect changes in position.
Embedded within this gelatinous layer are tiny formations of calcium carbonate, called otoliths. When a person moves or changes head position, these otoliths, responding to gravity, shift their position. This subtle shift in the otoliths alters the positions of the delicate filaments of the hair cells. This mechanical perturbation subsequently opens ion channels within the cell membranes, triggering a process of depolarization and creating an action potential that is promptly transmitted to the brain along the vestibulocochlear nerve, signaling our orientation relative to gravity.
Dynamic balance, conversely, is responsible for allowing a person to sense acceleration and maintain equilibrium during movement. This critical function is managed by the three semicircular canals, which are uniquely angled at right angles to each other, forming a three-dimensional sensory system. At the end of each canal is a slight enlargement known as the ampulla, which contains numerous cells with filaments grouped in a central area called the cupula.
When a person changes acceleration, the fluid within these canals, known as endolymph, rotates according to the momentum of the head. The inertia of this fluid changes with acceleration, which in turn affects the pressure exerted on the cupula. This pressure change causes the ion channels within the hair cells to open, leading to depolarization. This signal is then passed to the brain along the vestibulocochlear nerve, informing it of our rotational and linear movements. Dynamic balance also plays a vital role in maintaining stable eye tracking during movement, a reflex known as the vestibulo-ocular reflex, which demonstrates the integrated nature of our sensory systems.
6. **Embryonic Journey: How the Ear Forms**The development of the human ear during embryogenesis is a remarkable testament to intricate biological processes, with each of its three distinct structures – the inner ear, middle ear, and outer ear – originating from different germ layers: the ectoderm, endoderm, and mesenchyme. This complex, coordinated development ensures that all components are meticulously formed and integrated to achieve the ear’s sophisticated functions.
The inner ear is the first to begin its formation, starting around the embryo’s 22nd day from two thickenings in the ectoderm, known as otic placodes, on either side of the head. Each otic placode subsequently recedes below the ectoderm, forming an otic pit, which then closes to create an otic vesicle. This entire nascent mass is eventually enveloped by mesenchyme, which differentiates to form the protective bony labyrinth, the robust housing for the inner ear’s delicate structures.
Around the 28th day of development, parts of the otic vesicle begin the crucial process of forming the vestibulocochlear nerve. This nerve develops into bipolar neurons that are destined to supply sensation to the key sensory components of the inner ear, including the semicircular canals, the macula of the utricle and saccule, and the organ of Corti. This early neural connection is fundamental for the future transmission of auditory and balance information to the brain.
Further differentiation occurs around the 33rd day, as the otic vesicles begin to specialize. Posteriorly, they develop into the structures that will become the utricle and the semicircular canals. Anteriorly, the vesicles differentiate into a rudimentary saccule, which eventually matures into the saccule and the cochlea. A significant connection forms during the sixth week, as part of the saccule gives rise to and connects with the cochlear duct via the ductus reuniens, a critical link for fluid circulation and sound processing.
As the mesenchyme surrounding the cochlear duct undergoes differentiation, three distinct fluid-filled cavities emerge: the scala vestibuli, the scala tympani, and the scala media. While the scala vestibuli and scala tympani are filled with an extracellular fluid called perilymph, the scala media contains endolymph. The development of the vestibular membrane and the basilar membrane is vital, as they effectively separate the cochlear duct from the vestibular duct and the tympanic duct, respectively, maintaining the distinct fluid environments essential for auditory transduction. The molecular regulation of this process is largely controlled by homeobox gene families like Pax, Msx, and Otx, with Shh, secreted by the notochord, acting as a master gene.
The middle ear and its components arise from the first and second pharyngeal arches, distinct from the inner ear’s development. The tympanic cavity and the auditory tube develop from the first part of the pharyngeal pouch, specifically from an area that will also contribute to the pharynx, forming a structure called the tubotympanic recess. The ossicles – the malleus, incus, and stapes – begin to appear during the first half of fetal development. The malleus and incus are derived from the first pharyngeal arch, while the stapes originates from the second, with all three ossicles developing from the neural crest.
Unlike the inner and middle ear, the ear canal of the outer ear originates from the dorsal portion of the first pharyngeal cleft and is fully expanded by the end of the 18th week of development. The eardrum itself is a sophisticated tri-layered structure, composed of ectoderm, endoderm, and connective tissue. The auricle, the visible external ear, forms through the fusion of six specialized hillocks. The first three hillocks, derived from the lower part of the first pharyngeal arch, form the tragus, crus of the helix, and helix. The final three hillocks, originating from the upper part of the second pharyngeal arch, give rise to the antihelix, antitragus, and earlobe. Initially, the outer ears develop in the lower neck region, but as the mandible forms, they gracefully migrate to their final, higher position, level with the eyes, completing their anatomical journey.
7. **Understanding Hearing Loss: Causes and Solutions**Hearing loss, a condition that can significantly impact quality of life, manifests as either partial or total insensitivity to sound. It can arise from various factors, including injury, physical damage, congenital diseases, or physiological causes, each affecting different parts of the ear’s intricate system. Understanding the type and cause of hearing loss is the first step towards effective management and potential restoration.
When hearing loss is a direct result of injury or damage to the outer ear or the middle ear, it is precisely categorized as conductive hearing loss. This means that sound waves are not being efficiently conducted to the inner ear. Common causes for this type of impairment include a physical blockage in the ear canal, often due to excessive earwax, or issues with the ossicles, such as them becoming fixed together or being absent entirely. Perforations, or holes, in the eardrum can also significantly impede sound transmission, leading to conductive hearing loss.
Another frequent cause of conductive hearing loss is middle ear inflammation, such as otitis media, which can lead to a fluid build-up in the normally air-filled tympanic cavity. This fluid obstructs the ossicles’ ability to vibrate freely, thereby reducing sound conduction. For cases involving damage to the middle ear’s eardrum and ossicles, a surgical procedure known as tympanoplasty is often performed. This operation typically uses grafts from muscle fascia to reconstruct an intact eardrum or involves the placement of artificial ear bones to substitute for damaged ones, effectively rebuilding a disrupted ossicular chain to restore sound transmission.

8. **Congenital Abnormalities: When Development Takes an Unexpected Turn**While the ear’s development is a marvel of precision, sometimes congenital abnormalities can occur, presenting challenges from birth. These anomalies, particularly those affecting the auricle, are not uncommon and can range from minor variations to significant malformations. For instance, children may be born with abnormal ear canals, low ear implantation, or more profound conditions like atresia, where no auricle is formed, or microtia, characterized by an extremely small auricle. These conditions often arise when the auricular hillocks, critical for outer ear formation, do not develop properly, or when the ear canal fails to channelize correctly.
Such developmental deviations are more than just cosmetic; they can significantly impact a child’s hearing. Inner ear congenital anomalies, for example, are frequently linked to sensorineural hearing loss and are typically identified through advanced imaging techniques like computed tomography (CT) or magnetic resonance imaging (MRI) scans. It’s crucial for parents and caregivers to understand that the inner ear’s development is largely separate from the middle and external ear, meaning an anomaly in one part doesn’t necessarily imply issues in others, though combined anomalies can occur.
Middle ear anomalies can also arise from errors during the complex process of head and neck development. Conditions like the first pharyngeal pouch syndrome can associate middle ear issues with the malleus and incus structures, or lead to non-differentiation of the annular stapedial ligament, which is vital for the stapes’ function. These anomalies, alongside temporal bone and ear canal irregularities, can contribute to both sensorineural and conductive hearing loss, underscoring the interconnectedness of the ear’s components and the complexity of its embryological origins.
For children over five, reconstructive surgery is often considered a viable option to address hearing loss stemming from these congenital issues. The initial medical focus is always on assessing the baby’s hearing and the precise condition of the ear canal, middle, and inner ear. Based on thorough test results, reconstruction of the outer ear can be planned in stages, with concurrent preparations for any necessary repairs to the deeper parts of the ear. Cosmetic surgical procedures, known as otoplasty, are also available to reduce the size or reshape prominent ears, highlighting that interventions can address both functional and aesthetic concerns.

The intricate design and multifaceted functions of the human ear are truly astonishing, from its role in perceiving the world’s symphony to maintaining our very sense of balance. As we’ve journeyed through its anatomy, development, and various clinical challenges, it becomes clear that this small organ is a powerhouse of biological engineering. The surprising discovery of an ear print on a back door, while initially a prompt for home security, has opened our eyes to the ear’s incredible uniqueness, its profound impact on our daily lives, and its rich tapestry of cultural and evolutionary significance. Understanding and protecting this vital sensory system is not just about hearing the world, but about fully engaging with it, recognizing the silent sentinel that stands guard over our perception and equilibrium.


